unicorn
-
Posts
2,948 -
Joined
-
Last visited
-
Days Won
7
Content Type
Profiles
Forums
Events
Everything posted by unicorn
-
May I ask for the source of this information?
-
What percentage of these MAGA sycophants do you suppose have children/grandchildren in the armed forces? He calls our brave warriors "losers" and "suckers." " According to a 2020 Atlantic report, Trump reportedly made these comments when cancelling a 2018 visit to the Aisne-Marne American Cemetery in France, calling it "filled with losers," and allegedly referred to 1,800 Marines who died at Belleau Wood as "suckers"."... https://www.nbcnews.com/politics/donald-trump/john-kelly-confirms-trump-privately-disparaged-us-service-members-vete-rcna118543 https://www.theatlantic.com/politics/archive/2020/09/trump-americans-who-died-at-war-are-losers-and-suckers/615997/ "When President Donald Trump canceled a visit to the Aisne-Marne American Cemetery, near Paris, in 2018, he blamed rain for the last-minute decision, saying that “the helicopter couldn’t fly” and that the Secret Service wouldn’t drive him there. Neither claim was true. Trump rejected the idea of the visit because he feared his hair would become disheveled in the rain, and because he did not believe it important to honor American war dead, according to four people with firsthand knowledge of the discussion that day. In a conversation with senior staff members on the morning of the scheduled visit, Trump said, “Why should I go to that cemetery? It’s filled with losers.” In a separate conversation on the same trip, Trump referred to the more than 1,800 marines who lost their lives at Belleau Wood as “suckers” for getting killed...".
-
In my email, I specifically told him that I never have and never will cheat on my husband, and sent him two photos of my hubbie and myself, including one of our wedding pictures, and made it quite clear that I had no intention of hitting on him. I gave him my full name and address. He still hasn't responded, leading me to strongly suspect his pleas are a scam (already a bit difficult to believe without this confirming evidence). Many apparently are happy to blindly send him money, so easy pickings for him.
-
That being said, I'd vote for Puerto Vallarta (in Jalisco, the same state for which Guadalajara is the capital) being the most gay. It's certainly much more concentrated. The number of gay bars and restaurants may even be greater in PV than in MC. One would certainly say that PV is Mexico's "gay mecca." There are lots of luxury bus companies running the Guadalaja to PV circuit, and the road between the two cities (on the luxury lines) is quite good.
-
It's been over 24 hours since I offered both (1) the $100 coffee meeting, and (2) magician/entertainer gig for June pool party. No response so far, which makes me very suspicious that his story in asking for donations is a scam... 😉
-
Well, I sent him an e-mail. We'll find out if his story is probably true or not... 😉
-
-
My worst queueing experience was going through immigration for non-EU/EEA citizens at Lisbon Airport. Good thing I arrived at the airport 2.5 hours before departure. The line was over 1 km long and took almost 2 hours. Barely had time to reach my gate (no special line for business class, either).
-
I agree with you completely. I wouldn't consider this a charitable donation, but rather helping someone who's willing to meet a fan. Bonus points if I could get to know him better. I almost met Jason Caceres at a neighbor's party, but I was at a conference at the time. My husband told me he was there (he knows I'm a fan of the real JC 😁).

-
As you know, since you've read my posts, most of my charity goes to groups which help the unfortunate. Quite the contrary, if I end up helping him, he'll be the first "pretty" man I've helped. And as you also should know from my prior posts, I'm as gay and as atheist as they come. Since the Romans kept records of whom they crucified, and there is no record of him in Roman writings until well after his purported death, I find it unlikely that Jesus ever even existed, much less that he's still around. Also, I can't say I'm fully convinced he's the one supporting his parents. If he were to decline my offer for coffee, that would increase my suspicions that he's just making an easy buck off of his popularity.
-
I'm more inclined to be generous with people i know than with strangers... 😉
-
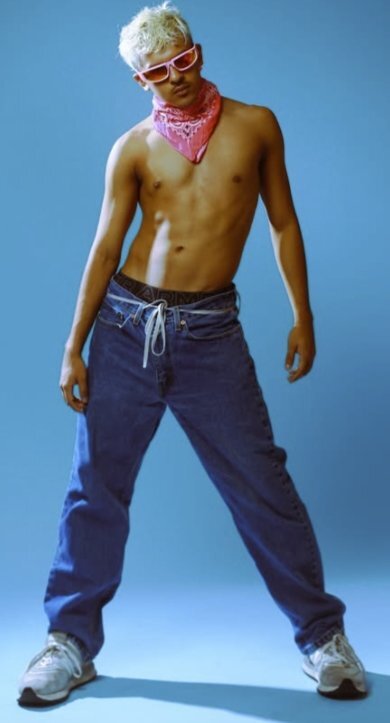
I've followed this actor, on whom I have a little crush, for a while, and I got this rather cryptic e-mail from him: https://www.patreon.com/posts/help-154038202?post_id=154038202 "Writing to you all to let you know that due to the health of my father declining, my mother and stepfathers divorce causing massive issues in finances, my car breaking down on me, my immense debt due to supporting my family financially and finally, my rapidly declining health which has caused me to "pass out" randomly (guess I'm stressed?) .. I have to ask for support to afford rent this month. I have been doing all kinds of side jobs, gigs, streams, selling personal belongings etc. to make it, but I.. don't have it this time. I can see myself failing to make this happen and so I wanted to reach out and ask for help and support if you have the means. I don't have much to offer you (other than my sincerest gratitude), I'm sure I can do a livestream to thank you, send each of you homemade cookies in the mail with a written, personalized letter (if you're okay with brown sugar, cinnamon, choc. chip cookies), mail you polaroid's... but I'm at my limit of what I can do. The number is above a thousand, but I would be grateful to even raise $5. Anything to help me find a step to stand up and continue forward...". https://www.famousbirthdays.com/people/skyler-seymour.html https://www.linkedin.com/in/yoskylerseymour/ If I can trust the internet, he lives quite near me (in Burbank). I'm thinking of handing him over $100 cash if he'll have coffee with me. He also works as a magician, and I suppose I could hire him for entertainment at my next pool party (June 13 or 14). To make it clear: I would shoot myself before I'd ever cheat on my husband, and am not interested in an intimate encounter--just to meet him. Sound reasonable?
-
I trust you're not insinuating that the two are equivalent...
-
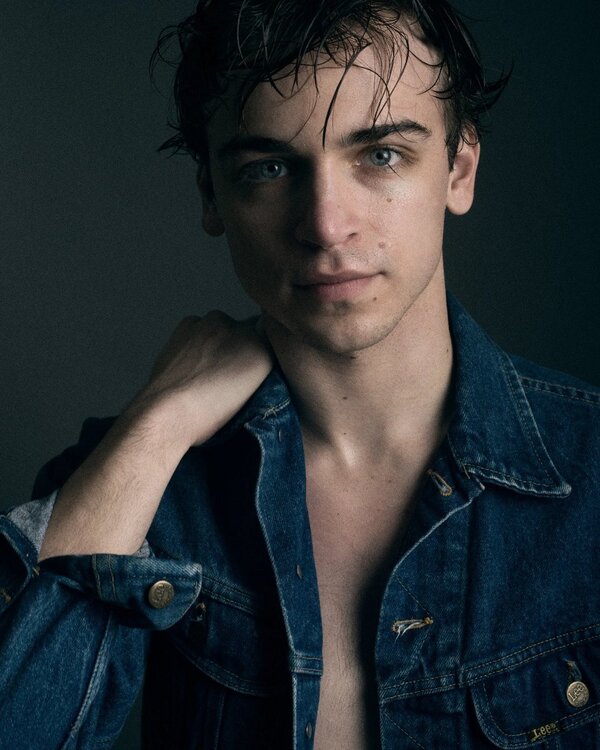
 No such luck looking for shirtless photos of some of the hunks on last night's show, Jesus Christ Superstar, seen at the Nocturne Theater in Glendale. An interesting cast, with several non-binary, including the person (using they/them pronouns) playing Mary Magdalene, and both non-binary and women playing apostles. The man playing JC was a hunk, and usually semi-shirtless on stage, but I was unable to find shirtless photos of him online (Diego Huerta-Gutierrez): I was only able to find a couple of shirtless photos of some of the dancers. Robbie Canevari: and Danny Castro:
No such luck looking for shirtless photos of some of the hunks on last night's show, Jesus Christ Superstar, seen at the Nocturne Theater in Glendale. An interesting cast, with several non-binary, including the person (using they/them pronouns) playing Mary Magdalene, and both non-binary and women playing apostles. The man playing JC was a hunk, and usually semi-shirtless on stage, but I was unable to find shirtless photos of him online (Diego Huerta-Gutierrez): I was only able to find a couple of shirtless photos of some of the dancers. Robbie Canevari: and Danny Castro:
-
Americans Yet Again Interfering With Foreign Laws
unicorn replied to PeterRS's topic in The Beer Bar
Maybe true, but that's up to the Finns. -
Unsurprisingly, you didn't read my OP carefully. While there are some gorgeous actors whom I follow, and will watch almost any movie, series, or short video they're in (such as Jason Caceres), in this case I was alerted to this show by e-mail, and my decision to go to the show was made (and tickets purchased) prior to seeing the photo of this cast member. There are even many times I see an actor at a show (or a barihunk at the opera), and will look him up for J/O photos after I get home. I remember a few years ago seeing another actor, Sean Grandillo, at another one of my favorite Rodgers & Hammerstein musicals, Oklahoma!, and falling in lust for him. I looked him up on my Playbill, and found some nice J/O photos when I got home. https://www.famousbirthdays.com/people/sean-grandillo.html https://www.facebook.com/p/Barihunks-100067732580746/

-
I don't understand your posting. I go to musicals to enjoy the singing and dancing, not because I intend to jack off in the theater while focusing on one of the cast members. And I gladly paid $200 for my two tickets, not worrying about the $5.50 per gallon we're paying over here in California, thanks to Donny Dementia. However, when I do see an handsome actor, I do search Google Images to see if there are shirtless pix I can use to J/O. There are a lot of "actors/models" here in LA. Which reminds me of that delightful soft-core porn movie:
-
Looks as though he's quite limber, too! 😍

-
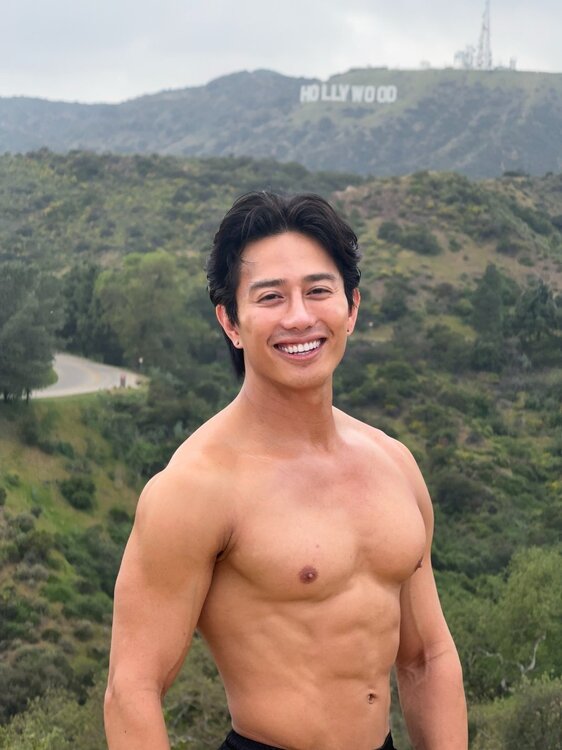
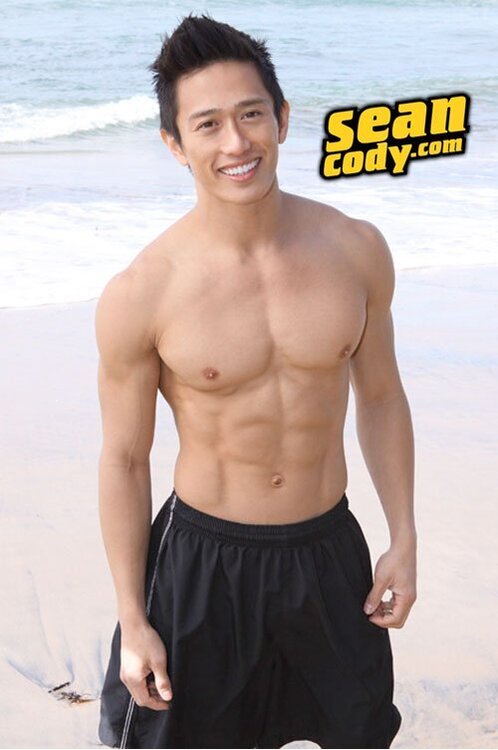
I was looking up a show recommended by an email of a musical I like, Flower Drum Song. In looking up the cast, one cast member immediately caught my eye: Joven Calloway, a member of Actors' Equity Association. I looked him up on Google Images to see if he had at least shirtless photo to which I could jack off. Boy, did I hit the jackpot! Not only does his Facebook account have lots of shirtless pictures, but it also includes links to multiple adult websites such as OF, JFF, and Sean Cody! In all of my horny years of looking up cast members in mainstream shows, I can't recall getting such a treasure trove! Do you every look up cast members for shirtless photos? Have you ever been surprised to discover a porn career in addition to a mainstream career? https://www.eastwestplayers.org/flower https://www.facebook.com/jkabobs/ https://linktr.ee/Jkabethandale https://www.famousbirthdays.com/people/joven-calloway.html



-
Also reminds me of a local (Los Angeles) story in which the Los Angeles Times found out that people were being paid to make false sex abuse accusations against the county of Los Angeles for cash: https://www.latimes.com/california/story/2025-10-16/sex-abuse-fraud-claims-la-county-victims "...Austin Beagle, 31, and Nevada Barker, 30, said they were trying to sign up for food stamps this spring when someone offered them a background role outside a county social services office in Long Beach. They thought the gig seemed intriguing, albeit a bit unusual. The offer came not from a casting director, but a man hawking free cellphones. The filming location was, oddly enough, a law firm in downtown Los Angeles. Maybe this was how actors were recruited here, they figured. The couple had recently moved from the remote ranching town of Stinnett in the Texas panhandle, and the recruiter seemed to appreciate their Southern drawl. They hopped on a bus, excited to make $200 between them. “They said we’d be extras,” said Beagle, who was unemployed at the time. “But when we got to the office, that’s not what it was at all.” The couple said they arrived at the lobby of Downtown LA Law Group. A Times investigation published earlier this month found seven plaintiffs represented by the firm who claimed they received cash from recruiters to sue the county over sex abuse, which could violate state law. Two said they had never been abused and were told to manufacture their claims...".
-
Found the ideal entertainment for my birthday party
unicorn replied to forrestreid's topic in The Beer Bar
https://www.guinnessworldrecords.com/news/2021/6/minnesota-teen-reclaims-record-for-largest-mouth-gape-664425 -
Sergio Fernandez: https://www.facebook.com/reel/1468677708199535
-
Found the ideal entertainment for my birthday party
unicorn replied to forrestreid's topic in The Beer Bar
You realize he's not gay, and lives in Northern Ireland? -
The point is that you simply choose to believe the alleged victims (in fact, you label them "victims" rather than "alleged victims," totally discounting any possibility you might be wrong). The human tendency to believe victims should be tempered by a willingness to examine facts, and not just statements. Currently, there is zero supporting hard evidence. One would be hard-pressed to even estimate the chance that these accusations are true (or false). At least if they were to test the out-of-wedlock children's DNA, they could show that the odds aren't zero that Huerta is being truthful. Of course, this wouldn't show whether or not the sex was consensual--just that sex between the two did happen. The fact of the matter is that neither you nor I know whether these allegations are truthful. Is she just trying to cast herself as a victim? Trying to improve her reputation after giving up two out-of-wedlock children for adoption? One piece of fact that makes me a bit uneasy at taking the accuser at face value is the fact that she claims two episodes of unwanted sexual intercourse (though in one case she says she was "manipulated" into consenting), and became pregnant each time. Even if Chavez was extremely unlucky, and happened to time the sex (both times) during the 1-2 days before ovulation, there's still only a 10-30% chance of pregnancy resulting in a live birth each time: AI Overview The probability of pregnancy from a single act of unprotected intercourse with a fertile woman varies significantly based on timing, ranging from nearly 0% outside the fertile window to approximately 10-30% during the most fertile days (1–2 days before ovulation). On average, the likelihood is about 3-4% per act of intercourse over a full cycle. The New England Journal of Medicine https://www.nejm.org/doi/full/10.1056/NEJM199512073332301 So even if we give the most generous interpretation of the data, that he happened both times to have sex with her during her two fertile days per cycle, and that the odds are 30%, not 10%, that still gives the odds of becoming pregnant both times to be 30% X 30%, or 9%. Outside the peak two days, or if we take the middle range of estimates, the odds drop dramatically. 9% is simply the maximum odds, with the most generous interpretation of the data, of two episodes of sexual intercourse during the fertile window resulting in live births. (I should also note that Huerta was in her 30s both times, hardly a woman's most fertile years) Even if the out-of-wedlock children are shown to be Chavez's, these data would make one have to consider the likelihood that his two children are more likely to have resulted from multiple (presumably consensual) sexual acts, rather than from two unwanted ones. There is little disincentive to falsely accuse, as prosecutions against those who falsely accuse are rare. In Huerta's case, the odds are zero, since she didn't make these accusations under oath, so could not be prosecuted for perjury. This article describes a rare case in which the false accuser was prosecuted: https://www.prosecutorintegrity.org/pr/99-of-false-accusations-go-unpunished-center-for-prosecutor-integrity-asks-why/ "99% of False Accusations Go Unpunished.... Nikki Yovino of New York falsely accused two football players at Sacred Heart University of rape. The woman later admitted that she had lied to gain the sympathy of a prospective boyfriend. As a result, Yovino was sentenced to one year in prison, plus two years of probation... One of the falsely accused men, Malik St. Hilaire, sadly recounted, “I went from being a college student, to sitting at home being expelled, with no way to clear my name. I just hope she knows what she has done to me. My life will never be the same. I did nothing wrong, but everything has been altered because of this.”...False allegations are widespread in the United States. A national survey sponsored by the Center for Prosecutor Integrity found that 8% of Americans — 11% of men and 6% of women — report being falsely accused of sexual assault, domestic violence, or child abuse. The 8% figure represents 20.4 million adults (2)...".
-
Obviously, neither you nor I has enough (nor will we ever have enough) information to believe or disbelieve the accuser. It's certainly problematic when one has the mindset that the accused has to "disprove" allegations in order to be considered possibly innocent, especially among those whose minds is already set. That's the definition of mob mentality (and many have been lynched because of it). How would you like it if you were accused of a crime, and told no one would believe you unless you could "disprove" the allegations? I guess that still happens in some countries--one would hope not advanced societies. Accusers get plenty of sympathy, not grief, especially from those close to them. It also wouldn't surprise me if Cesar Chavez day were renamed Dolores Huerta Day. At this point, one is deluding oneself if one thinks one knows the truth. It's really unknowable at this time. One can only wonder: why bring up these accusations now? If it were true that bringing up the accusations results only in "grief," there would be no motive. No one is accusing her of lying. There's no way to tell either way. There have certainly been examples of false accusations, including the blatant lies discovered in the Duke Lacrosse players' case, which ruined innocent men's lives. While not as clear-cut, the Kobe Bryant case was probably another such case. I can only wonder why Huerta is bringing this up over six decades later, and over three decades after Chavez's death. I find the overnight rush to take down his statues and murals troubling.