unicorn
-
Posts
2,920 -
Joined
-
Last visited
-
Days Won
7
Content Type
Profiles
Forums
Events
Everything posted by unicorn
-

Do you enjoy "What do they look like now?" articles?
unicorn replied to unicorn's topic in The Beer Bar
I was also reminded of the before and after photos as I looked at the photo my husband has of me on his dresser. It's of me in my mid 20s. When he shows it to friends, the photo often gets over-the-top reactions like "Oh, my God!", as if I'd turned into some kind of ogre. 😄 😁Well, there are few who survived into their 60s still looking as hot as in their 20s. Brad Pitt and Tom Cruise are the only two I can think of, off-hand... -
The Murders of Rob Reiner and his Wife: and the Issue of Anger
unicorn replied to PeterRS's topic in The Beer Bar
In my first post on this string, I wrote: "I hope I'm reading this incorrectly, and that you're not hinting that the parents are in any way responsible for their own deaths...". To which you directly responded: "With much regret I am indeed hinting this...". The fact that you later said that you were not the one who came up with this theory doesn't change what you wrote.You're simply backtracking now. -
Do you enjoy "What do they look like now?" articles?
unicorn replied to unicorn's topic in The Beer Bar
Gaak! Corey Feldman is a good advertisement against the ravages of substance abuse. At least he lasted longer than his fellow substance abuser and "friend" Corey Haim. -
Do you enjoy "What do they look like now?" articles?
unicorn replied to unicorn's topic in The Beer Bar
Fabio appears to have aged decently well, IMHO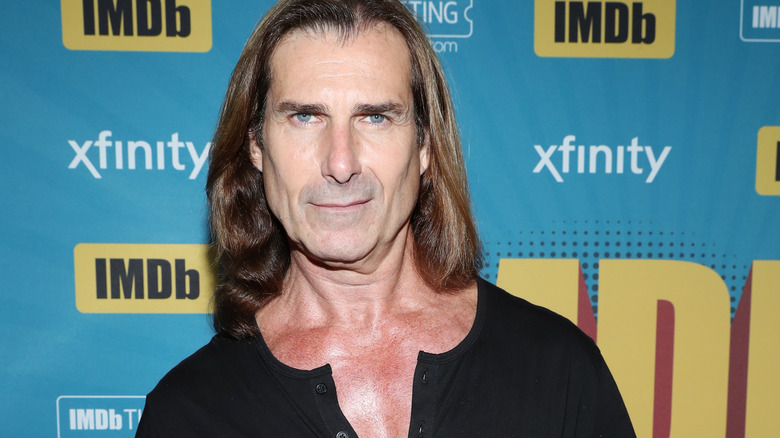
-
The Murders of Rob Reiner and his Wife: and the Issue of Anger
unicorn replied to PeterRS's topic in The Beer Bar
In your original post, you stated the parents were responsible for the murders due to "...a misunderstanding on the part of the boy’s parents on how to deal with such very substantial on-going substance abuse, and a steady build-up of anger." You later stated stated that the parents "took their son to endless doctors, psychiatrists or whoever they believed qualified and thereafter took their words as gospel," which, to me, implies that you blame them for placing too much value on professionals' advice. It appears as though the parents originally followed the professionals' advice and later maybe didn't. If you want to clarify your beliefs, would you clearly state your position? Was the parents' error in following the professionals' advice too closely, or was it due to their ultimate (apparent?) rejection of such advice? -
-
It's ironic that there are many foreign speakers on this trip (from Spain, Germany, Belgium, Colombia, etc.) whose English is easier for us to understand than the Australian's. And English is the Spaniard's 3rd language (he grew up speaking Catalan in Mallorca, then learned Spanish in school, and later English).
-
Not really. In the US this can only happen when both houses of Congress, the Presidency, and the Supreme Court are all controlled by the same party. In a parliamentary system, the political leader and the leader of the legislature are one and the same, so it is always the case (especially since the legislatures in such systems are almost always unicameral--the House of Lords doesn't really have any power). There have certainly been times when in the US, all 3 branches were controlled by the same party, but never by led by a sociopathic criminal con-man before. Even Thatcher wasn't that nutty. In a parliamentary system, there really are no checks and balances. In Hungary, Orbán has unfettered power, with resulting consequences. Trump could easily happen in any parliamentary system. It would be.a mistake to think it can't happen. A lot of damage can happen in 2 years, but at least Congress will probably be able to put the brakes on Trump's criminal endeavors in another year or so. Had the Democrats been able to pick their candidate, this horror probably wouldn't have befallen the US. Unfortunately, Biden's dementia and ego prevented him from understanding he was in no condition to run again, much less rule. Disaster ensued.
-
I'm from the Far West (live in Los Angeles, grew up in Oakland), I don't pronounce merry and marry the same, thought Mary and marry are only slightly different.
-
Which parts?
-
One has to pronounce Mandarin Chinese carefully to say "Is Mom cursing the horse?" Māmā mà mǎ ma? 妈妈 骂马吗?
-
My husband was startled upon seeing the current appearance of the legendary actress Shirley MacLaine

-
We just had a Australian guide give us a tour of a former whaling village in the South Shetland Islands. The Australian habit of pronouncing almost every vowel like a long "I" made it at times difficult for us to understand him. For example, he pointed to a structure and said "This is where they had their whiles...". It wasn't until he finished his sentence with "so they could obtain fresh water," that I understood he was saying "wells," which in Australia is pronounced the same as "whales" and "whiles" (it had occurred to me that the structure was too small to contain whales). 😉
-
I must admit that at the current time, it would be nice to have a monarch or his representative call for a new election. My understanding though is that this almost never happens in any of Charles III's realms, so even that theoretical advantage doesn't seem to exist in practice. I suspect that a new Congress will put the brakes on Cheeto Benito's (and his lackey Speaker Mike Johnson, the closest we have to a Prime Minister) shenanigans in another year or so. At least the two years of unfettered power will show the US public what doofuses the Republicans are, and there won't be anyone else to blame. It would also be nice for the President of Israel to call for a new election, but it doesn't look as if that's ever going to happen. When the legislature and the country's political leader have unfettered power, disaster can occur, and this is almost always this is almost always the case in constitutional monarchies--prime ministers run the legislature. I have a feeling that despite Republican monkey-business attempts to dilute Democrats' votes, Johnson will lose the speakership in another year. At least in the US system, the legislature can put the brakes on the country's political leader. Johnson's too much of a pussy to get his nose out of Don the Con's ass. This is the first time Americans have elected a bona-fide convicted felon and con-artist to lead our country. Not all Presidents have been great, but this is the first time we've had a dictator--at least until the '26 elections.
-
When Australia wants to become a republic instead of a monarchy, they have only to vote and choose to do so. Until then, they can continue bowing and curtsying to their royal families. Charles III is still their king. Americans rejected the monarchy two and a half centuries ago:
-
The Murders of Rob Reiner and his Wife: and the Issue of Anger
unicorn replied to PeterRS's topic in The Beer Bar
I never accused @PeterRS of lying. I found his posts, however, ambiguous in their meaning and easy to misinterpret. If what he meant to say was that the parents erred in NOT following professionals' advice, then we agree completely in this matter. -
The Murders of Rob Reiner and his Wife: and the Issue of Anger
unicorn replied to PeterRS's topic in The Beer Bar
Wow, wow, wow. So you actually believe that Nick Reiner (and his parents and you) knew better than professionals with "diplomas on their walls," who actually looked at the science of the matter and studied the issues for years, how to treat himself? News flash: almost all addicts lie. I think that the evidence is pretty plain. The fact that the parents rejected knowledgeable professionals' views and advice is what led him to relapsing and ultimately to kill his parents. The fact that the three of them were so sure they knew better than the experts how to treat him is what led to the tragedy. Similar fates have happened to many people who eschewed the advice of medical professionals because they knew from their faith that medical professionals didn't know what they were talking about (such as Scientologists and Christian Scientists including Jim Henson). Although the parental instinct may be to cover up, comfort, and enable all of the messes addicts get into, this behavior is ultimately to the detriment of well-being of the addict, to say nothing of those around the addict. While addicts love it, enabling is ultimately counter-productive. For the most intransigent addicts, a good, long prison sentence is ultimately what will help them change their behavior. Some addicts need more time in jail than others. Paris Hilton was a spoiled brat, doing drugs, driving under the influence, etc. Fortunately for her, her judge knew she needed some time in jail to reflect on her behavior. When she drove while her license was suspended for a DUI, she finally served 23 days. Although she continues to be a bit of a wild woman, her behavior has improved since being behind bars. -
Trump Solves Thai-Cambodian Conflict - Or Does He?
unicorn replied to PeterRS's topic in The Beer Bar
I'll never forget the words of those who killed him: "It's a pity he can only be killed once!". Ceaușescu was indeed a monster. I felt the same when Jeffrey Dahmer was killed. -
Russia cuts off internet access to Rainbow Railroad
unicorn replied to unicorn's topic in The Beer Bar
There's more to getting asylum than getting a tourist visa. RR not only helps foreigners get the right visas (say, to Canada), but also helps support them once they're safe on Canadian (or other) soil, with housing, job assistance, and so on. -
Putin has cut off internet access to Rainbow Railroad, an organization which helps members of the LGBTQ+ community in hostile countries (such as Russia, obviously) leave the country and get asylum elsewhere (most commonly Canada): https://www.rainbowrailroad.org/the-latest/russia-blocks-rainbow-railroads-website-cutting-off-a-critical-lifeline-for-lgbtqi-people This is an organization I fully support, and also has the full backing of charitynavigator.org as an honest and efficient charity. Hopefully they can at least access the website with a VPN? I don't know if the government has a way of punishing those who access the website via VPN?