Riobard
-
Posts
4,127 -
Joined
-
Last visited
-
Days Won
19
Content Type
Profiles
Forums
Events
Everything posted by Riobard
-
The Phase3 trials assess for baseline SARS-CoV-2 status and stratify accordingly for analyzing efficacy and vaccination response. Pfizer/BNT had 6.2% with prior infection. J&J had 9.8%. These research subjects are identifiable, and clinical sequelae associated specifically with CoV exposure history are evaluable. However, the rarity of clotting that leads to acute illness may not yield much additional info by going back to that cache of serum samples that is small relative to real-world uptake. Noorchashm did have a very compellingly persuasive 5 minutes with Tucker Carlson of Fox News. So his concerns are not totally “buried”. He did hold back, though, in pointing out the obvious, that proximal profit margins would depreciate if those recovered from CoV were bypassed for inoculation.
-
[Delete]
-
Dunno. Whenever Brazil 2.0’s many off-limits aspects, too many to list right now, are cleared, I guess, and flights are greenlit. Apparently as a Canadian I cannot transit through USA returning from Brazil, Panama connections are currently wonky and likely also subject to restrictions, and the EU is recommending all its member countries join the ones banning flights to and from Brazil.
-
See, I cannot submit ... guess the system sees me as exclusively ativo and will allow other ‘characters’ of questionable repute. ;>D
-
My Twitter feed reveals case reports about the syndrome, eg one just published in NEJM, that suggests causal factors other than the past/recent CoV infection one. It’s probably too complex an issue to attempt to unravel in discussion here on the Board. Also, the author Noorchashm does not list an institutional affiliation. Though it would likely be important to follow his simple to execute recommendation. You could spend days following feeds of high-profile clinician scientists on this ... Eric Topol, Eric Feigl-Ding, Hilda Bastian, loads of others, and get many varied opinions.
-
I touched on this theme this here in the forum months ago when referring to ADE ... antibody-dependent enhancement of disease, and I had added that the FDA EUA submissions had referenced it ... that it is a consideration about which little is known viz COVID. Know your natural immunity status by antibody testing and your CoV infection status by viral testing (as many cases are asymptomatic or paucisymptomatic), at the point of inoculation planning prior to actually pursuing artificial immunity, at least prior to the first (sole) shot of a 2-dose (single-dose) regimen. What is cray-cray is those jabbing you protecting themselves from transmission because you may be infected and contagious at the time. The meta message being: you are about to be inoculated possibly too late against a disease that you may currently have, but seeing as you are here, roll up your sleeve. Why would you want the huge payload of immune system stimulation with a compounding of simultaneous virus and a viral facsimile? Additionally, some of the limited vaccine stock could be (have been) deployed to those without any protective immunity, saving more lives at a point of product scarcity. The population percentages of those with protective natural immunity can be quite substantial where prevalence has been high. This doctor authoring the piece suggests screening for nucleocapsid antibodies after the fact, investigating the clotting, as regular antibody testing would conflate natural and artificial immunity. For pre-vaxx purposes ... note that I am far from being an expert ... I believe the generic antibody tests are fine. I think they target the antibodies specific to the viral spike protein. My personal go-to has been the Roche CoV antibody assay. Mind you, I tend to get sore throats likely related to allergies so that is one feature that has propelled me at times into getting (free) local viral tests, followed occasionally by the pricey antibody test I have to pay for in Quebec. I also checked that I did not have natural infection antibodies prior to receiving my first dose in an all-blind placebo-control RCT. I quarantined assiduously to ensure I would not have been recently or currently infected at the point of inoculation.
-
There’s a difference. I just cannot remember what it is. And inertia prevents me from investigating and trying to roll back to basic. Maybe I will at the next annual charge.
-
Straight Men Have Gay Sex... Are They Still Straight?
Riobard replied to Lonnie's topic in The Beer Bar
My sense is that if you need 343 pages with countless references the answer remains: don’t know. Which is good for the married men ... can keep their wives off-balance. -
I think my use of Grindr Xtra has averaged to about $100 per hour and I have never had an actual meetup.
-
It puzzles me at this point why nomenclature such as the vaccine and the shot(s) is still utilized. It’s as if one goes to the fast-food restaurant and has the hamburger ... when in a rush and a pinch it is a good option to go to a fast-food restaurant and have a hamburger.
-
We are all in it together. ;>) BTW, how do you add emoticons in post text? I always get a warning it is not permissible.
-
USA is calling halt to Johnson and Johnson Vaccine
Riobard replied to TotallyOz's topic in The Beer Bar
A huge amount of moving parts and we will likely see a lot of comparative metrics. Say we keep it to risk of blood clots among those inoculated and the proportion of clot-poz vaxx recipients dying. And vet out dumb analogies such as crushed by a vending machine. Risk of acquiring CoV by age, risk of dying from COVID stratified across age (in Canada .064% or 1-in-1,570 by reported CoV incidence age 20-49; or .002% when estimating true case incidence). Risk of blood clots associated with CoV itself, itself also a quantifiable probability, degree to which clots occur and contribute to mortality variance among the infected, adjusting mortality rate according to case incidence ascertainment bias (undercount) as I did for Canada, etc etc. Risk of blood clots associated with other elective products such as birth control pill or smoking, risk of dying of blood clots associated with vaccine if post-vaxx surveillance and pre-emptive intervention were to be added, controlling for comorbidity in assessing risk of COVID death among those <50 and in assessing risk of clots among vaxx’d <50, etc, etc. Haven’t had my morning coffee yet, but in the spirit of adding illustrations ... the death table, not the clot metrics, is from CDC.


-
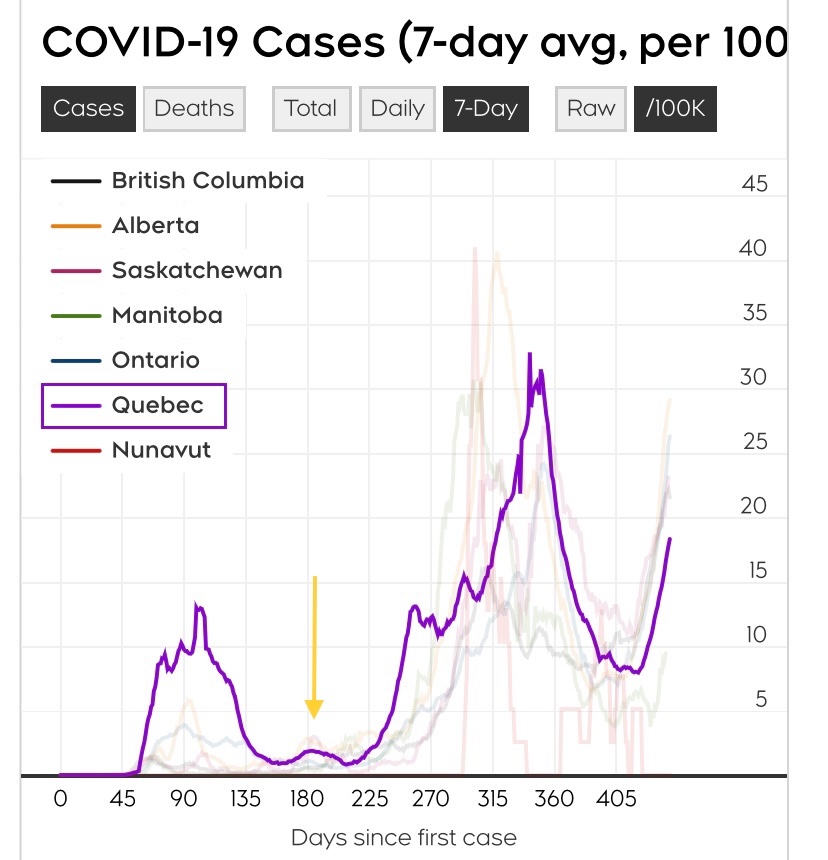
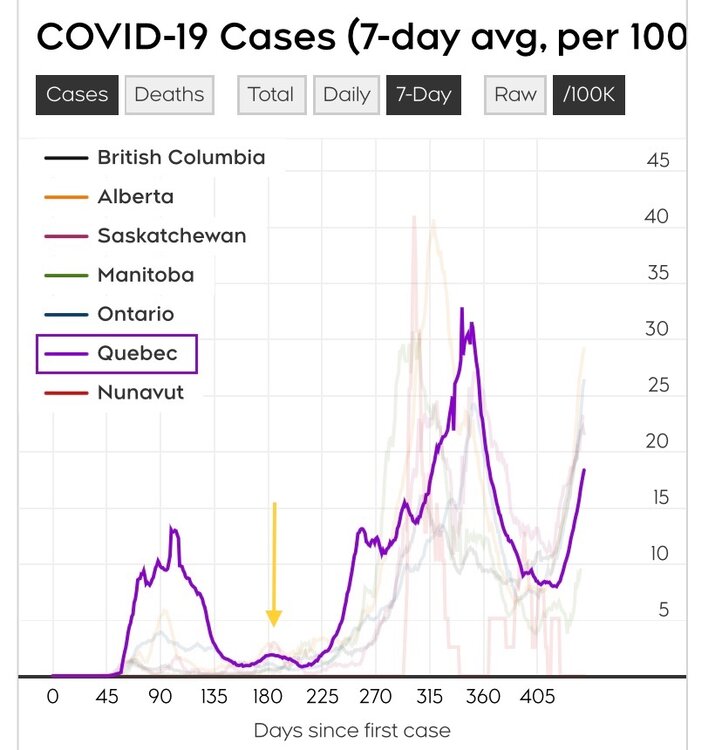
I take back what I wrote several weeks ago about Montreal. Our case incidence is trending up again, now at a level that would have to settle down quite a bit to reach last summer’s nadir levels (yellow arrow) that allowed partial re-reopening. However, the goal of one vaxx dose for everybody that wants one seems achievable by July 1st. The tide may turn.
-
JOYFUL JAUNT SANTO DOMINGO
Riobard replied to BlkSuperman's topic in Latin America Men and Destinations
Oops. It’s only compatible with iOS and Mac; comes automatically with iPhone, iPad, etc. -
JOYFUL JAUNT SANTO DOMINGO
Riobard replied to BlkSuperman's topic in Latin America Men and Destinations
I hope that one realizes that when one hole has had enough and needs a break there are other hole options. @BlkSuperman, do you have the iMovie app? I have it on my iPhone. One can easily merge the individual clips into one seamless video. Sorry if this suggestion seems bossy ... we beggars should not try to be choosers. Let me know if you want to be walked through it, that is, if you are off your back long enough. -
USA is calling halt to Johnson and Johnson Vaccine
Riobard replied to TotallyOz's topic in The Beer Bar
The average person cannot grasp the probability math. -
Delete ... sorry I must be back my old terrible habit of hitting Quote when I meant to click Edit ... edit used to be at the bottom of the field. AFAIK, the impulsive false step is irreversible once clicked. That is why some of my posts look like full quotes, I guess. Let’s consider it rehearsal for driving you all insane to the point where there will be no getting around reducing the two Latin American sections to one. ;<)
-
Delete
-
-
Correction on earlier wording ... it is Gamaleya Institute’s Sputnik V.
-
OK I read the Yucalandia piece. It is poorly structured and written, confusing and unclear at times, apart from evaluating its scientific accuracy and merit. And I am neither a virologist/immunologist nor reading the vast written material related to the theme of this article. I have the capacity to grasp some of this, but I don’t understand where he is getting some of his figures. He is also tossing in the cons of various products that we already know about, while skirting over the pros of the ones to which he is negatively predisposed. I think the message he(?) wants to get across is that vaccines built upon the entire virus, as opposed to exclusively the spike protein or subsections of the spike protein, are superior in terms of protection against inevitable mutations. The question itself is relevant and I had wondered myself a few months ago what would be the implications of mutations for the spike protein subunit model, containing no actual viral genetic material, for the vaccine I received experimentally. However, where the argument loses me is that the receptor-binding domain of the spike protein is key for this disease. With genetic drift (ie, spike-specific variants), that key element is going to be a moving target whether for products that zero in on the spike protein and its components or for products based on whole virus. Mine is a simplistic critique based on second-guessing the author’s intent and somewhat all-over-the-map message. With case-control effectiveness trials now emerging, comparing retrospectively those newly infected in terms of having been vaccinated in the real world or not, in contrast to the reverse (efficacy: vaccination followed prospectively by infection incidence tracking), it is progressively more and more difficult to keep up with all the data.
-
-
I only mentioned pinned topics to guide you to see where my new unpinned topic landed in sequence, but not in the place I wanted. I think you are saying that the one forum intended to be open without membership is now restricted and perhaps the content would be lost if you removed it ... not being able to transfer the threads posted to date in a way to integrate the two into one LatAm option.
-
-
I am currently less pessemistic about CoronaVac in Brazil. Will elaborate today or soon. I struggle to assess efficacy meaning and accuracy unless the study results are formulated using the detailed report model framework that researchers are using to apply for USA FDA EUA. So I would have to drill down, and consume mucho vodka, to try to figure out Gamalaya Institute’s vaccine product Sputnik (Sputnik 2 may be its name if I recall). Note that various Brazilian states and municipalities are going rogue while Anvisa (their FDA equivalent) is holding firm on its standards. Since their last approval of 4-5(?) candidates for Phase 3 trials provided up until last summer, not one candidate has been authorized for study. The only one approved for efficacy research since last August was just greenlit: Quebec and Durham NC’s Medicago protein subunit type with GlaxoSmithKline’s adjuvant. There are also many other wheeling and dealings among politicians, science institutes, and third-party national and/or foreign companies behind the scenes in Brazil. I am not about to try to call an outdoor steeplechase race, in an electrical storm, with a few Zola Budds but no Usain Bolt among the competitors. (Sorry Zola, if it weren’t for that pesky South Africa variant ...)