Riobard
-
Posts
4,124 -
Joined
-
Last visited
-
Days Won
19
Content Type
Profiles
Forums
Events
Everything posted by Riobard
-
It is, obviously, but we are at this juncture dealing with the bigger picture globally. I think that most people by now are aware how 67% effectiveness stands up compared to 90+%. And that if you can snag a product of that lower efficacy caliber purely in terms of its capacity for case and severity reduction when nothing else is available you take it. Low levels of vaccination hesitancy somewhat compensate for lesser efficacy, as does the ability to avoid delays in follow-up booster doses within the initial vaccination cycle. Chile is using as much of 3 of the vaccines you listed as it can get. Should it have waited to administer approximately 90% of vaccinations, the percentage attributable to CoronaVac given over the past few months, and substituted them with products with greater than 67% effectiveness yet some with complex cold-chain logistics, whenever they trickled in over their Autumn, trading off lives for snubbing a product that is now showing well above the threshold of efficacy for authorization? I don’t think so. I believe the take-home is that you need vast inoculation uptake, combined with their approximate existing 20% natural immunity within the population, in order to see results, outcomes that are likely already unfortunately compromised by immunity-escape and more contagious variants. Chile also tests at quite a high level, so the average true degree of case severity decreasing is not necessarily reflected in rolling new case incidence; reduced hospitalization and mortality is essentially a surrogate marker for vaccination apparently reducing symptom burden. Moreover, vaccine effectiveness calculations are often artificially lowered by relatively high levels of natural immunity in the population, as is the Chilean case. The true effectiveness is probably better than the recent 67% reported. Similarly, CoronaVac effectiveness is a metric comparing infection case variables between those inoculated, and not, with CoronaVac. Since close to 5% of the population not vaccinated with CoronaVac is partially or fully vaccinated with products clinically higher in efficacy rankings, the true effectiveness of CoronaVac in isolation is, again, artificially deflated because the two groupings do not start off with the same proportions of baseline immunity.
-
Based on the long thread there, now gone unless the sites boot up again, on what could go wrong and hypotheses about how to deal with an intestate situation and salvage the sites, it’s head-spinning. But there was a basic contingency plan for some involved to maintain communication and continue problem-solving attempts behind the scenes if the sites were to go dark. Moderators of sites like this would do well to have a simple mostly inactive social media account (Twitter the easiest because you can create as many accounts as you like without revealing your true identity), for backup communication about what is happening.
-
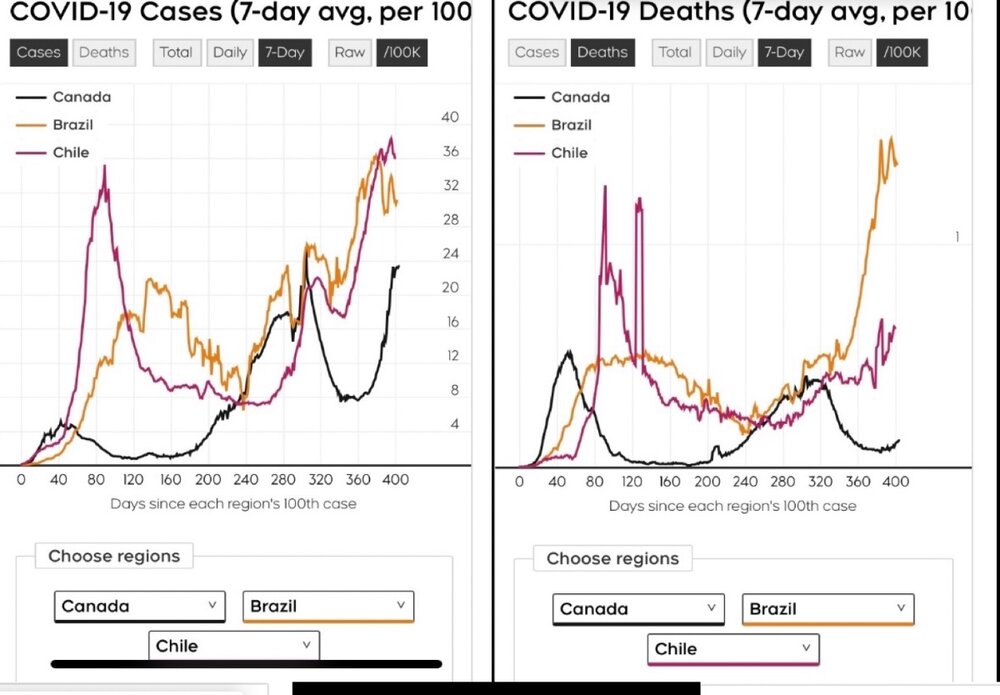
They are not incidence rates. They represent the amount of reduction in incidence for the vaccinated compared to the non-vaccinated for millions vaccinated thru Feb and Mar. Effectiveness is a calculation much like efficacy, the latter in a controlled research trial, the former applied in the real world setting. If somebody showed you these metrics and you were asked to try to explain the differences in incidence (per 100K population) between Chile and Brazil, without knowing their vaccination status history, it would be reasonable to assume that Chile had a far more advanced vaccination campaign because the new case incidence is similar but reduced mortality, a primary desired endpoint of inoculation, is quite pronounced for Chile. It is about half, two-fifths that of Brazil, with almost identical current infection case incidence trend. Brazil’s and Chile’s case fatality rate historically tracked similarly to their respective incidence rates but now Chile’s mortality relative to case incidence is considerably lessening. These are more crude comparisons that corroborate more systematic epidemiological research.
-
Things move quickly. That report is already outdated. Here are the recently updated data. ‘Partial’ means prior to second dose of CoronaVac. The counterintuitive rise in case incidence is an artefact of reckless behaviour, among the approximately half of population not yet fully inoculated; and for those vaxx’d, with the standard period required for individual immunity buildup following inoculation not yet achieved, in context of more contagious P1 variant. Otherwise, CoronaVac is having a positive impact, poses minimal adverse events, and is welcomed by the people. CoronaVac was never intended to be single (partial) dosing. The results underscore that the full dose cycle is imperative. [Similarly, complete municipal vaccination of Serrana using CoronaVac, SP, BRZ is yielding dramatically beneficial results] [The article uses the term ‘the Chinese vaccine’, conflating Sinovac’s CoronaVac with another company’s product, that of Sinopharm, being utilized and now manufactured in UAE.] CHILE:

-
I thought that as well, reasonable interpretation, until I realized that over the last 6 days of surveillance the ratio of cases fully vaxx’d to non-vaxx’d is 8:25, not a good showing. If the ratio for vaxx:prevaxx were known that might explain it. The problem is not knowing that ratio and its progression over the 40 days. But as more are vaxx’d, the less non-vaxx’d there are to take a percentage share of daily diagnoses. I realize now the uptake is somewhat staggered as there are cases late in the period among the <14 days following 2nd dose. Thanks for the input. The MOH report will diminish in relevance and I doubt the MD will reply to my questions seeing as they are buried among hundreds of comments in his social media feeds. LOL. Folks have also asked for even basic rough info on the vaccination products used. I suppose he does not want more people then going off and trying to calculate efficacy. He put this report on FB but not Twitter and does not answer any comments.
-
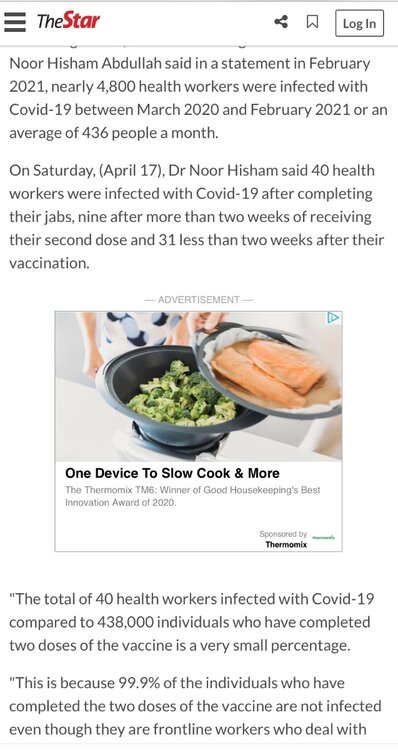
So I put this as a comment, one of hundreds made by others on this report, on the gov’t doctor’s FB: The denominator is 426 vaccinated HCWs, not 430K+ HCWs in the nation of which some of the whole collective of HCWs received vaxx. 244 non-infected were included as it is a small cohort inoculated with 1st dose on the same day (presumably)?? This makes the CoV rate among the HCWs correctly vaccinated 2.1%, not 9+31 vaccinated out of 430K+, which would be negligible. What is totally confusing is that in the later days of the 40-day period the share of infections is high among those that had been fully vaccinated for at least 2weeks. The design needs to be clearly elaborated in order to interpret the pie chart and histogram. Does ‘none’ mean non-vaccinated or non-infected? If it means non-vaccinated, why were so many partially or even fully vaccinated HCWs infected relative to the non-inoculated? And that makes 9/142 = 4.9% of the fully vaxx’d HCWs infected.
-
[Delete]
-
Sorry, @spoon, the confusion is not resolved. Another article says the 438,000 vaccinated is in total pop, not specifically HCWs. Also, the guy put 244 non-infected into the calculation so the denominator has to be 426, not 438,000 ... this puts the vaxx’d HCWs at 2.1% infected at the point immunity should have been conferred, suggesting it was a small cohort all vaccinated on the first of the 40 days and followed for CoV status. There is no way 438,000 could have been simultaneously vaccinated on March 7th. So this now means a contradiction in the screenshot above from The Star. He said the fully properly vaccinated HCWs had negligible incidence. There is now a paywall so I cannot return to it. My worry is that he was so intent on underscoring the importance of additional vigilance following the period of vaxx up to sufficient protective immunity that he royally messed up the data.
-
I just sent the Malaysian doctor my questions via Messenger. —— Addendum: I found the answer, maybe the doctor will need to correct the apparently misinterpreted tweet from the other source.
-
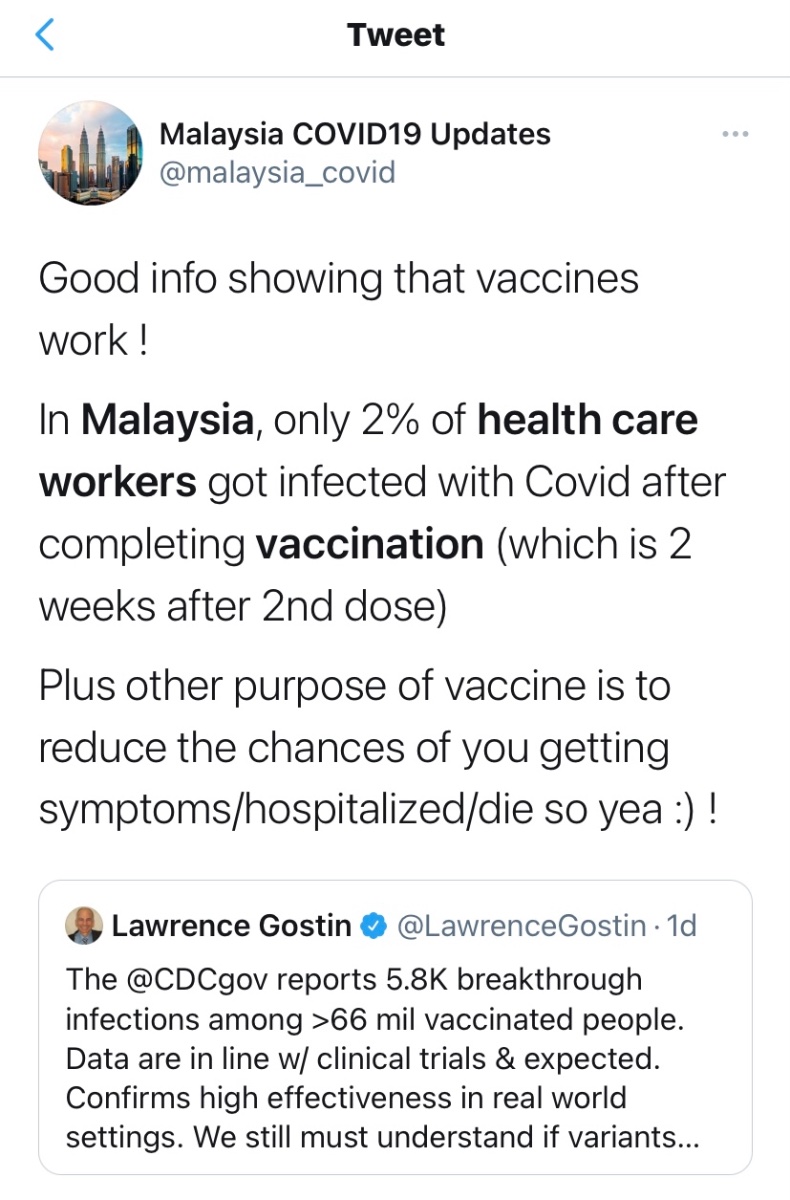
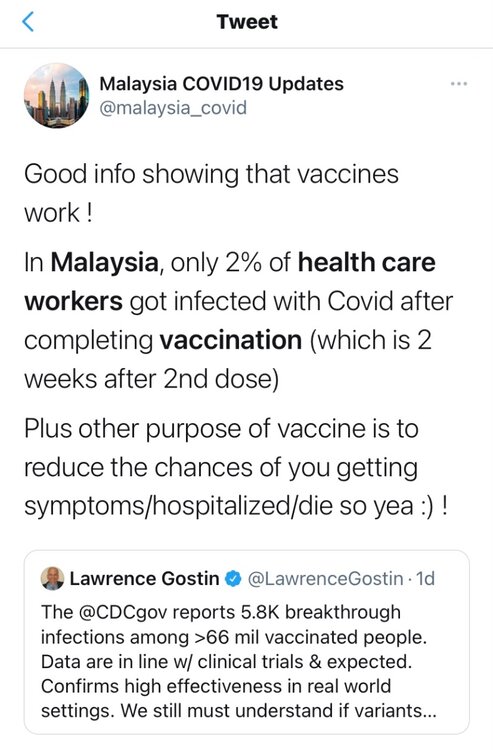
But this Tweet from what appears to be an official local epi Twitter site, @spoon ... then they posted a USA example of breakthrough infection. Is it meant to be sarcastic? If so, why would they add the part about preventing severity and death? Maybe the doctor did not present the actual HCW Ndenominator because it was not precisely known. On the doctor’s Facebook page (Noor Hisham Abdullah) one English comment on the low incidence after all, but it follows some Malay comments so I cannot really figure out that thread. BTW, in either case the numerator is 182, not 426. ————
-

-
[Sorry, the system would not allow my script after I quoted you in the previous field.] The rate (proportion) of infection among the fully vaccinated HCWs is 2.1% over a brief time period. The rate within the vaccination assignment arm in Pfizer\BNT over a longer time period is .043%. Vaccination among these Malaysian HCWs did not work well because they were 48 times as likely to acquire CoV compared to those vaccinated in the efficacy trial and were 13 times as likely to acquire CoV as the (mostly) unvaccinated general population. Vaccinated HCWs in the Brazilian CoronaVac efficacy trial also had a similar incidence, close to 2%. However, that was consistent with the unvaccinated general pop. Yet it suggests that in the real world Malaysia HCW setting the mRNA products were no better than CoronaVac. Though no placebo control or non-vaxx’d HCW group to truly assess the effectiveness in the Malaysia study. Perhaps the Malaysian HCWs were in a high concentration of incidence. They really take a hit. How many people would want to risk a 1/50 chance of going to work and getting infected shortly following the recommended vaxx dose cycle? CDC just reported an estimated .009% breakthrough infections among those fully vaccinated, over 2,000 times these Malaysian HCWs.
-
-
@spoon, vaccinated, not vaccinated, post-vaxx duration aside, 43% CoV incidence among HCWs is 269X background cumulative incidence for Malaysia’s genpop (.16%) over the same 40 days. The higher rates in HCWs in other studies are usually up to 2-fold, not well over 200-fold. That would cripple any health care system. The report and illustration do not make sense. It seems impossible to me unless the HCWs had volunteered to be exposed to almost inevitable infection. Was it a ‘challenge’ study? The wording says “were infected” ... semantically that could mean they were planfully exposed as opposed to ‘they acquired infection randomly’.
-
Breaking: Rio Lock-down & Curfew
Riobard replied to Riobard's topic in Latin America Men and Destinations
Wise move. Break the circuit. It’s the UK variant and it may be inflated by cross-border travel from Cambodia. Thailand will have to revert back to 14-day quarantine; 10 days is too leaky wrt to a strain that is more contagious, with a longer contagion period, than original wild-type CoV. This is likely partly the cascade effect of an identifiable quarantine breach in Cambodia in February, with cases surging there now about 25% higher rolling incidence than Thailand after having had a negligible volume of cases since the pandemic commenced. Thailand scaled back quarantine duration April 1st. They didn’t see the newer smaller leaves coming and switched to a rake with tines spread too far apart. Hindsight is 20:20. It’s all happening very quickly. I would not be surprised if this scuppers Thailand’s plan for local cluster vaxx for the tourism spot Phuket in order to deploy the limited supply to infection hotspots. -
I am returning to this basically because I had questioned the value of CoronaVac. Not that I should be considered an influencer either way, but I should point out that this vaccine now seems to be proving itself reasonably well in overall real-world effectiveness, 67%, in Chile and is acquiring much acceptance particularly in Brazil. Also large reductions in hospitalization and death. The good PR reduces hesitancy there and that can compensate somewhat for lesser efficacy relative to some of the other vaccines. It also appears to come with minimal side effects / adverse events. I did not want to trash-talk it a while ago and then fail to report more recent news about it as well as my increased optimism about this Sinovac product.
-
Addendum: the occurrence of the rare clots of concern is not that common with COVID apparently. So there are clots and there are clots. But 10x greater risk with COVID than vaxx for the worrisome clot types with the long 4-word label , according to Oxford U.
-
FullSizeRender.mov
- 1 reply
-
- 2
-
-
I found it on Hooman Noorchashm’s recent Twitter feed. But the feeds of a few ‘armchair’ yet qualified clinicians and epidemiologists that I and many others respect, as they seem to relentlessly jump on every COVID story that comes out and unpack it objectively, without an apparent personal agenda of their own, make no mention of this one. ——- Because the thromboembolism factors are quite widespread in COVID itself, and the onset of associated problems occur on a variable timeline, retrospectively testing for nucleocapsid-specific antibodies that confirm previous infection prior to vaccination among those vaccinated presenting with the clotting syndrome won’t necessarily tell you whether the clotting is precipitated by vaccination as opposed to the clotting emerging latently, temporally coincidental to post-vaxx, as an aspect of having had COVID. It may be that the rare clotting shows glaringly following vaccination because vaccination is an easily identifiable singular antecedent. In contrast, the same clinical phenomenon, while known, is obscured or buried among many other symptoms or complications requiring primary attention among folks sick with COVID. So you won’t have had a news cycle that was just sayin’: BTW, you def don’t want COVID cuz apart from the risks of needing intubation you may get antibodies clumping platelets together. Also different political animals.
-
Brazil Retirement Questions 2021
Riobard replied to bucknaway's topic in Latin America Men and Destinations
And that is why Brazilian ‘trade’ should be a bona fide tax-deductible medical xpense. -
Breaking: Rio Lock-down & Curfew
Riobard replied to Riobard's topic in Latin America Men and Destinations
Rio mayor now infected, and symptomatic again, with New CoV after having had CoV Classic 11 months ago. -
On another note, as somebody that pushed for health education literature for the general public that did not exceed, for example, the Flesch-Kincaid 5.0 literacy level, the brief CDC quote above fails. OK OK, somebody may now take a swipe at me. LOL. But this forum is not representative of average community literacy.
-
The Phase3 trials assess for baseline SARS-CoV-2 status and stratify accordingly for analyzing efficacy and vaccination response. Pfizer/BNT had 6.2% with prior infection. J&J had 9.8%. These research subjects are identifiable, and clinical sequelae associated specifically with CoV exposure history are evaluable. However, the rarity of clotting that leads to acute illness may not yield much additional info by going back to that cache of serum samples that is small relative to real-world uptake. Noorchashm did have a very compellingly persuasive 5 minutes with Tucker Carlson of Fox News. So his concerns are not totally “buried”. He did hold back, though, in pointing out the obvious, that proximal profit margins would depreciate if those recovered from CoV were bypassed for inoculation.
-
[Delete]
-
Dunno. Whenever Brazil 2.0’s many off-limits aspects, too many to list right now, are cleared, I guess, and flights are greenlit. Apparently as a Canadian I cannot transit through USA returning from Brazil, Panama connections are currently wonky and likely also subject to restrictions, and the EU is recommending all its member countries join the ones banning flights to and from Brazil.