Riobard
-
Posts
4,127 -
Joined
-
Last visited
-
Days Won
19
Content Type
Profiles
Forums
Events
Everything posted by Riobard
-
For all the trash talk about China’s vaccines, WHO with its stringent review process just signed off on Sinopharm’s BBIBP-CorV, the sixth product thus far to receive the stamp of approval, though recommending for under age 60 for now. The decision about Sinovac’s CoronaVac comes next week. The media’s call on it is a toss-up. I think it will be greenlit. The recent follow-up effectiveness trials all indicate meeting the 50% threshold or better. Brazilians and Chileans have been keen to queue up for it and there have been no indications of serious adverse events. Sadly, President Bolsonaro continues to badmouth China and much damage control is required. The Chinese cannot seem to take in stride that he is essentially insane. —-

-
Au contraire ... it’s common knowledge that the vaccines are assessed using the correct stepped-up phase methodology that depends on a study subsample getting sick and with higher numbers getting the illness. If the group subjects not receiving the vaccine are spared infection the efficacy is zero-to-inadequate infection risk reduction. No vaccine approved. The effectiveness of first-line vaccines already reduces the volunteerism willingness of research subjects to stay with the defined protocol. Huge drop-outs of placebo controls. Add the disincentive of freedom limitations for research subjects when a majority of the population essentially lobbies for unique privilege that was facilitated by those volunteers but is not accessible to them, why not just go out and squeeze a deuce into your closest essential worker’s corn flakes?
-
You can have vaccine passports required for most activities or you can sustain ongoing vaccine research & development utilizing the robust trial modalities that have yielded the inoculation options in the first place ... rescue vaccine interventions for which the notion of substantial immunity has sprearheaded the basis for formal recipient certification that privileges such activities. You cannot have both. The one paradoxically undermines the other. Short-term gratification is your agenda, or preservation of ‘gold standard’ research endeavours that may be continually required for a non-abating pathogen. Take your pick. Or use more common sense in determining alternatives prerequisite for actualizing privileged entry points into desired, renewed behaviour. It is more feasible to apply an overarching and more flexible range of validation for immunity or non-infectivity, all of which are preventive but not without their own unique flaws. The observer and subject-blind trial recipients of neither vaccine nor placebo will qualify for vaccine certification, and why would they volunteer, altruism grinding up against sacrifice of privilege? Surely the risk of non-intervention arm assignment is enough to have to endure. This is not Yellow Fever, the vaccination development and implementation strategy all laid out and stable. Without sufficiently longitudinal and solidly populated placebo-control randomized assignment research, the essential trial prospects that are left might include noninferiority SARS-CoV-2 vaccine comparison trials or challenge trials in which subjects are exposed to coronavirus infection following an experimental vaccine. The optimal structure for creating and testing vaccine candidates gets compromised. The essential foundations should be preserved.
-
Oh, good! You were spared infection thus far and your upcoming advantage is dosing at an interval that pays greater and faster dividends for protection.
-
We only see in the media vaccine efficacy expressed as relative risk reduction for study subjects able to benefit from vaccination. In contrast, absolute risk reduction considers the entire population and the infection attack rate based on the per capita background infection incidence over the same time period in which the research occurs. Absolute risk reduction tends to be ignored because the metrics appear to be unimpressive, all less than 2% for the currently predominant EUA product shortlist, and might de-incentivize vaccine uptake. It is much lower because the actual risk of infection without vaccination is quite low; the problem is the deleterious impact of a case. Moreover it is a moving target predicated on constantly changing infection incidence, whereas study efficacy has the illusory appearance of stability ... it doesn’t really have stability though, judging by the broad range of confidence intervals for the single-value efficacy metrics presented. Absolute risk reduction is utilized as the denominator, with the numerator held as a constant, the value 1, for calculating the number needed to vaccinate to prevent one more case of SARS-CoV-2. The difference in background infection incidence explains why the clinically less effective AstraZenecaOxford vaxx requires 78 persons vaccinated whereas PfizerBNT requires 119 vaccinated in order to offset each single new case. The former had a higher background population infection incidence. As community vaccination progresses, the background rate of infection will pivot from the entire population as denominator to the sub population of infection ‘susceptibles’ as denominator. In other words, although population incidence declines the new case incidence among those without natural or artificial immunity has the potential to peak at rates heretofore unseen for the general population throughout the pandemic. Much of this depends on the attack rate among the unvaccinated and assumes that they may generally tend to cluster together more (like seeks like). The subgroup number needed to vaccinate for new case prevention will shrink. By that time, the vaccine with greatest clinical efficacy will predominate on offer for the infection susceptibles, as simultaneously the number needed to vaccinate to prevent new cases will have declined within that specific subset. The greatest true effectiveness is based on the higher the relative risk reduction (ie, study efficacy) and the lower the number needed to treat to prevent each additional new case. These considerations will likely play a beneficial role for a potential second-wind surge towards the finish line for whatever the threshold of community immunity will be. —— Coles Notes version: The greater one’s risk of infection, the greater the personal and collective benefit of vaccination. Inoculation among those with high susceptibility to infection spills over preventively to the entire population at a greater level than for those vaccinated at an overall lower smoothed-out risk of infection. It’s shitty if early rollout vaccination is declined by essential workers, because their acceptance confers the greatest population collective benefit. But even a lower vaxx acceptance by them compared to a higher non-essential pop acceptance can potentially yield a better overall protective benefit by the former for the overall public. Residual non-immune susceptibles, same idea, but there is at that point a much smaller proportion of the progressively immune population subject to infection risk posed by those that transmit infection, as vaccine breakthrough is low.
-
Let’s remember that there were vaccine breakthroughs of initial wildtype SARS-CoV-2 for BNT162b2 from the get go in pre-EUA research, and the ratio of moderate to severe cases was technically mathematically suggestive of no less probability of severe disease than was observed in the population at large. It is not the spectre of a new strain that necessarily inflated the potential for lethal infection. That can occur across all variants. The massive breadth of vaccination simply provides enough volume of vaccinated people to have COVID death lurking among them/us, albeit lesser rates.
-
It is highly unlikely there will be a legal mandate for obligatory vaccination even though it is the prerogative of authorities at many levels in Canada and USA to physically impose inoculation in certain contexts for the greater good of public health, all of course subject to mostly futile court challenges. However, there will probably be at most the appearance of a mandate based on privileges and restrictions that amount to the vaccine decliner being forced to cooperate for the sake of the same freedom, paradoxically, their insistence of which takes current vaccination refusal to the mat. I would expect that there will be defined categories of people more subject to freedom limitations, based on a stratified hierarchy of transmission vector factors. This could play out to whatever arbitrary yet fluid definition of overall community immunity creates the right balance of health & safety, as well as some degree of grudging non-optional tolerance for a microbial entity that is not amenable to negotiation. It is somewhat silly at this juncture to extend the ‘all talk’ to ersatz active mandate since many folks that desire vaccination do not yet have access to it. Eventually, the supply chain will have eliminated the previous absurdity of enforcing a theoretical concept that is presently far from a uniformly concrete intervention. Again, the enforcement idea is figurative.
-
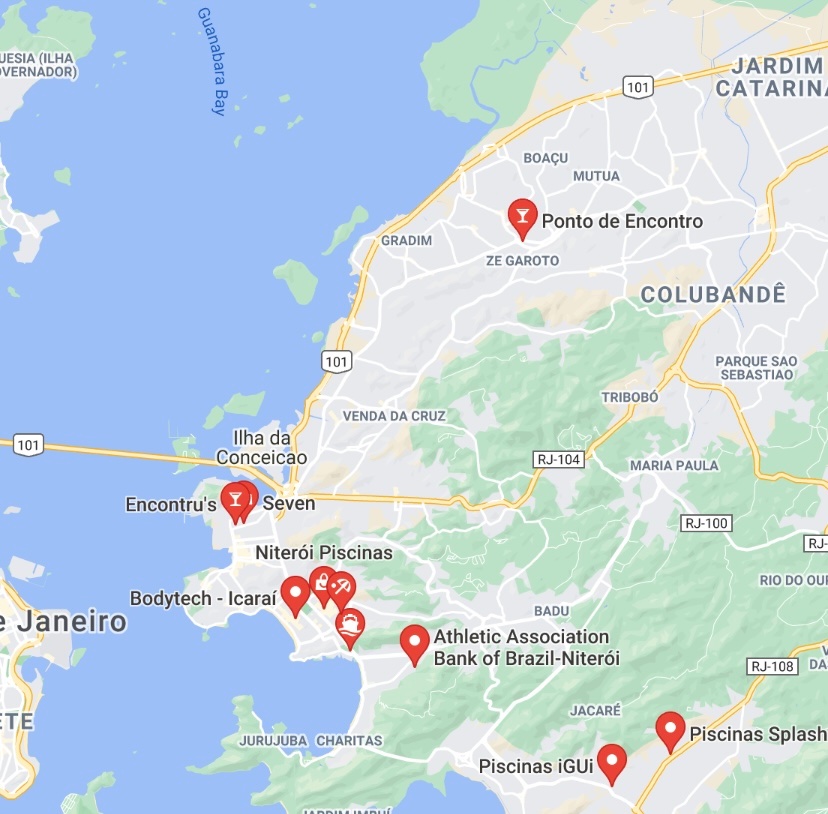
Ponto de Encontro (Sao Goncalo/Rio Vicinity)
Riobard replied to BrazilianBoiChaser's topic in Gay Rio De Janeiro
Reminder that the name may be confused with Encontru’s, gay complex closer to the ferry terminal. Don’t know if it formally has trade. Free entry for “boys” this coming Friday may be a clue, but other references are about “interactive boys”, so it may be about sex shows in the open. Somebody will have to take one for the team and report back, does not need to be a Sunday afternoon. I emailed out the critical question and will update if I get a response. Eventually this venue may be posted elsewhere here, so as not to highjack the thread. I put it here in case somebody plugs it into Über by name rather than specific address and ends up at the wrong destination.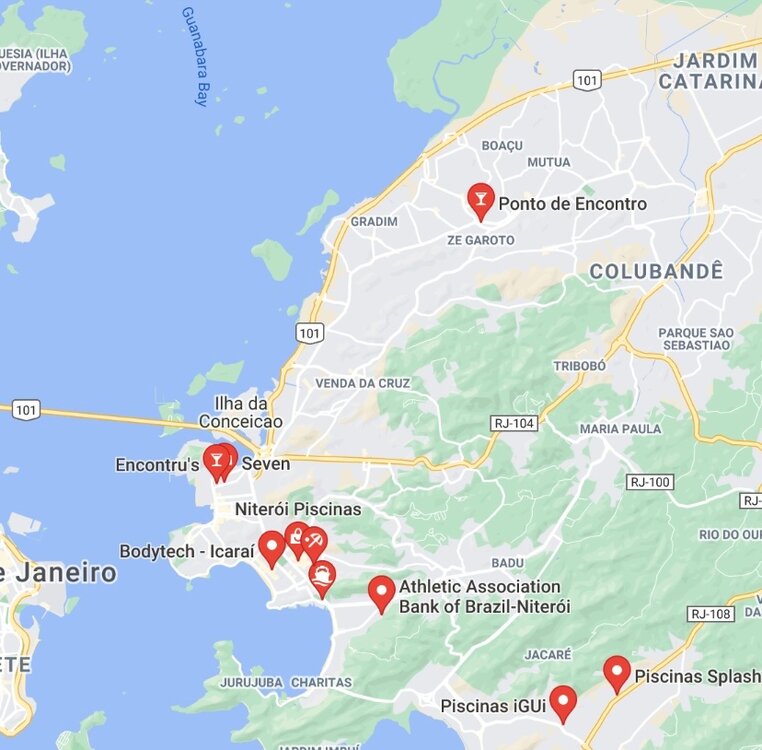
-
Seems like, outside of quarantine requirements I have not investigated, it’s either a 2-dose regimen necessitating a longer stay or two separate visits, or J&J single dose.
-
It is known from preliminary lab studies that the level of antibodies generated against the P1 variant by the mRNA vaccines is lower compared to original wildtype virus strain. The clinical implications are not known. Chile likely has P1 fairly predominant and just reported real world effectiveness for about 4.5 million complete dose2of2 CoronaVac inoculations. As they have data for about a half million full vaccinations with Pfizer’s BNT162b2 we may see some effectiveness metrics against the backdrop of some degree of P1 proportionality. Chile seems to have a very sophisticated database of infection surveillance, natural immunity, and vaccination uptake by product. The USA CDC will apparently soon be only monitoring vaccine breakthrough resulting in hospitalization or death. Chile is all in with CoronaVac and now with Sputnik V, siding with Russia against Brazil’s Anvisa rejection of the latter, but with enthusiasm in common with that of Brazil for the former. This could result in bypassing BNT162n2 as a product comparator if there if is not going to be much further use of it, a lost opportunity given that large scale mRNA vaccination where P1 currently predominates is unlikely elsewhere. I think that what is more relevant is, one, the relative vulnerability of being partially as opposed to fully vaccinated with either of the two mRNA’s. There is a significant gap in protection comparing dose1of2 and dose2of2, and many nations are delaying full vaccination. And, two, the known potential of vaccine breakthrough infection increasing with community case prevalence. The rolling incidence in Brazil is 7 times that of Dominican Republic.
-
Santo Domingo, The Land of Plenty, Part 1
Riobard replied to Arabcreamer's topic in Latin America Men and Destinations
I’ll plunk this news here, as it may be relevant for choice of accommodations. The country’s automatic CoV-inclusive med insurance for visitors arriving by air and going into hotel accommodations just expired, but is under review for temporal extension. If not extended, likely does not matter how digs are chosen. If extended, and if the incentivizing of free insurance provision by your host destination is important to you, you may wish to select hotel accommodations that are covered by the plan. -
Top Places to Retire 2021 for under 2500 USD per Month
Riobard replied to TotallyOz's topic in The Beer Bar
Another factor:
-
Or simply “Bubbles” if it was carbonated.
-
Santo Domingo, The Land of Plenty, Part 1
Riobard replied to Arabcreamer's topic in Latin America Men and Destinations
There is a precedent for Hispaniola being split down the middle. -
Apparently about 93% of the consumers are Brazilian, so I don’t think that the site is ‘cleaning up’ viz foreigner use, depending on the relative proportions. Non-Portuguese speaking users may prefer sites that don’t come with quirky translation mishaps. Though I doubt that the proportion of English speakers using Chaturbate is as low as 7% and I cannot comment on text-chat translation quality there. At first glance, however, CameraPrive has a lot more providers that appeal to me.
-
14-day quarantine mandatory for all arrivals in Thailand from May
Riobard replied to reader's topic in Gay Thailand
WHO reviews Sinovac’s CoronaVac today and makes its recommendation for granting emergency use listing. Fingers crossed. -
Santo Domingo, The Land of Plenty, Part 1
Riobard replied to Arabcreamer's topic in Latin America Men and Destinations
Thanks. Up to you, but I would advise you not rush in to openly share any of your social media account information here in the forum ... just yet. Maybe behind the scenes in DM. Take some time to get the lay of the land. You don’t have to find a middle ground for disclosure simply because you have been pressured and may feel a bit that you are withholding, thereby not being a ‘good sport’. -
That amounts to a 75% mark-up for my CameraPrive beef compared to a 34% mark-up for a Big Mac in Canada relative to its price in Brazil.
-
Yaaaas, you classy Pontifical forum bouncer, you ...

-
Santo Domingo, The Land of Plenty, Part 1
Riobard replied to Arabcreamer's topic in Latin America Men and Destinations
Post, don’t post. I’ll read whatever is added, but don’t expect Pom-Poms or backflips for encouragement. If I like it I’ll indicate same. -
Santo Domingo, The Land of Plenty, Part 1
Riobard replied to Arabcreamer's topic in Latin America Men and Destinations
[Delete] -
Santo Domingo, The Land of Plenty, Part 1
Riobard replied to Arabcreamer's topic in Latin America Men and Destinations
Guys, perhaps I’m mistaken, but I took this to mean a slew of direct messages put him off, with an indirect way of saying second thoughts about continuing the report. You’ll need to scroll up, the quote content keeps disappearing when I try to snip out the non-relevant part. -
Dumb question here. What’s the currency denomination? A few years ago I was in Brazil and looked into registering, had a bit of back and forth texting with admin. The fees were, for example, 15 reais for Brazilians for a ‘15’ charge, but as a foreigner it was going to be $15 USD, though that would mean even more in Canadian dollars. I wasn’t complaining, just inquiring, but the person got all defensive, suggesting I had it better and should be willing to pay multiples more. I don’t think they grasped the global Big Mac Index, where that burger costs only a bit less in USD in Brazil compared to America. Anyway, if I spring for, say, a ‘5 whatever’ or ‘100 whatever’ charge for one provider photo or chat listed at those ambiguous prices what exactly is the charge going to be on my statement? One reason I am extra curious, having written it off at that time when there were few guys on the site, is that a few lads I follow obsessively on social media, not strippers or escorts that I knew of, are now showing up!
-
I’m frequently now seeing on social media recognizable Brazilian guys, including those in the ‘trade’, showing up in the Mexican Riviera. Because it’s one of few countries they can currently visit? Any idea what their typical flight path is between Brazil and Cancun area?
-
I just assume there is always an element of risk, of lack of control over the privacy aspect of what I post, and that I don’t exclusively own my content. However, there is content I likely would not have posted if not retired, financially independent from employment connections, and essentially untouchable in terms of my professional affiliations being bitten in the ass. Similarly, I have posted content on these sites that I might not have written if an American residing in USA ... I realize that might be a bit of overkill in terms of worry.