Riobard
-
Posts
4,124 -
Joined
-
Last visited
-
Days Won
19
Content Type
Profiles
Forums
Events
Everything posted by Riobard
-
Given descriptions of the complex I suspect one of the stripper themes could be switched up. STOP, DROP your panties, and ROLL over. ;>I FullSizeRender.MOV
-
Yeah I read about it in their social media. I am there soon but had not planned on visiting the club. Perhaps this means the hot dancers (not hot due to fire of course) are more accessible for the duration. LOL
-
This was a DIY self-curated excursion utilizing city and regional public transport. Left accommodations in El Poblado at 06:15; arrived back at about 17:15 If questions, happy to respond.


-
Guatapé with El Penõl capture, Antioquia lake country; 2-minute reel: IMG_6255.MOV
-
They are certainly plentiful enough to line up as a groin-to-ass human centipenetration.
-
FullSizeRender.MOV
-
Yes, I have read the App is even worse than using the website version on one’s smartphone. I have not had a PC or printer in almost a decade. Anyway, good to know from you that the window is under 72 hours, providing more time for dealing with setbacks than the mere 24-hour window, considering door-to-door travel itself was 18 hours. COPA in Montreal said it was mandatory and are accustomed to apologizing about not being able to facilitate the task. I was not asked at JMC arrival but, as I said, passport was scanned and I assume was linked. Long queue; I was tired but had the advantage of being first off the plane and wait was but minutes. Suitcase immediately ready, and in bed at Hotel Movich Las Lomas next door 15 minutes later.
-
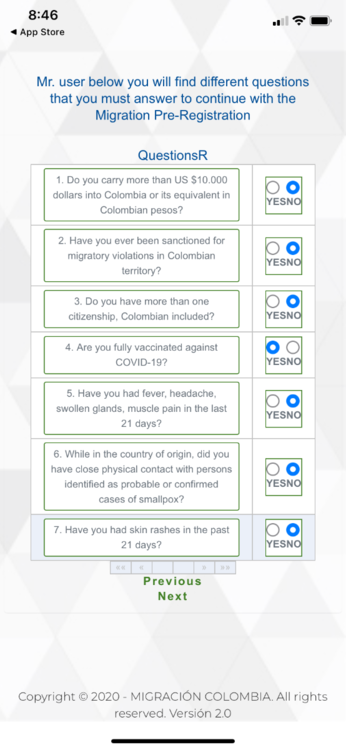
This online health declaration can be stressful. I had previously read about hassles and glitches getting to successfully completing it, as well as efforts to trouble-shoot. There are third party companies offering to assist for a fee! There are likely more experienced travel ‘paisaxperts’ here that will weigh in. First of all, the timing prior to departure is ambiguous. It is either 1-24 hours prior to touching down in Colombia, or possibly 72 hours (that makes more sense). I opted for completing it 23 hours prior to arrival, but a pop-up emerged suggesting no more than 72 hours prior to arrival. Which is it?! I asked fellow travellers in the Immigration queue in Colombia and nobody seemed to know. One must also need to complete it to depart Colombia. Since the initial form lasts 30 days, I wonder what fun and games will ensue upon trying to use the system again for a new purpose when the system already has me registered for arrival and might not free up a departure application. The airline in Canada emphasized it would absolutely be needed to board. I was late at night struggling with it prior to very early morning call for flight. I completed the form but received no “receipt” of acceptance or proof either within the site or by email. I understand there is no QR code. I will attach what it looks like, from someone posting it in Google images, so I don’t need to spend time redacting mine. I tried again several times but kept getting a prompt indicating I was already registered. Eventually, going back and entering a few dozen times to no avail, a receipt finally emerged a few hours later, within the application, not via email. Crisis averted and I was able to get at least a few hours sleep without worrying about navigating it again on check-in at the airport. Interestingly, it has recently added a VARV screening, also see attached. Good thing I am not prone to hives when frustratingly pulling my hair out meeting mandatory form completion and receipt proof that is elusive owing to system problems. I assume the Immigration officer accessed the declaration when scanning my passport upon arrival.

-
Barcelona (Thermas) 2019 latest recommendations
Riobard replied to joe2001london's topic in European Men and Destinations
Yes to your question. A booster dose overrides the expiry of the initial complete series and is itself not subject to expiry. Make sure you look up the Spain Travel Health form. I am pretty sure it is still required and while you can request it online ahead of time I think you complete it within 48 hours or 2 calendar days up to departure. I met the pre-booster criteria in May but I think there is a provision to identify all of your doses as you yourself need. You get a QR code, but bring other verification formats with you though likely not needed. However, there is lacking uniformity in Europe. It appears that Switzerland has imposed a 270-day expiry for a booster dose, and Germany has set this October 1st as the date at which a booster dose is mandatory even if 270 days from the initial series has not elapsed. -
You think I’m going for the Tântrica?! How VERY daaare you?! FullSizeRender.MOV
-
I wouldn’t worry about it. Sounds like you’re not. You’re delivering a package, a niche theme, not the total package accompanied by the soundtrack of Love Story. The genre wording is not a bait&switch, unlike a lot of profiles that don’t deliver what they describe or mostly just post links to other profiles for purchase consideration. The early foundation germane to the project was clear: persuading escorts oriented to discretion to be filmed doing your hole, and the idea growing inside of you expanding outside of you. It was always the fuck you’re facin’, not the face you’re fuckin’.
-
If face-covering is the default trade-off mode for actor recruitment I highly suggest more upscale apparel that has a bit more fetishistic potential as opposed to the exclusive interpretation by observers of obscuring identity for personal reasons, and snowmobile/dogsled-grade material at odds with the warm climate.
-
So my friend in Rio has Monkeypoxx
Riobard replied to bucknaway's topic in Latin America Men and Destinations
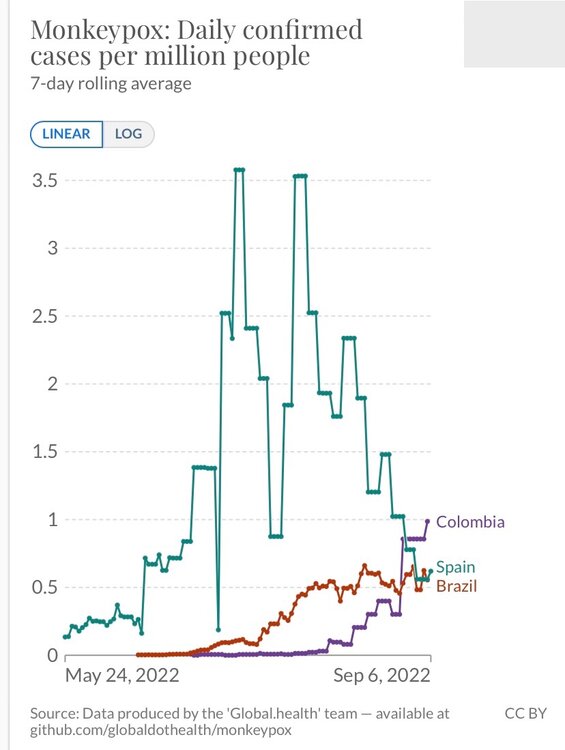
It appears to be more dire than that, but this point in time may not reflect the future. Cumulative to date is not as relevant a share of global count and higher case accumulations tend to be associated with subsequent drops in incidence. Brazil’s current rolling incidence is trending at 18% of the total global new incidence. However, the ratio is driven by declining incidence elsewhere. The trend has been for new case incidence to hover at a peak and then drop, irrespective of vaccine access. Brazil’s incidence has held steady for 6 weeks following an earlier rapid 10-fold increase. Fingers crossed for them. Obviously vaccine inequity has played a part and administration of MVA-BN would help either prevent incidence increases or drop the curve more quickly than is tentatively predicted. -
I would suggest quantifying the ratio of generally non-lucrative likes to actual purchases to date, in such a way that is consistently measurable irrespective of mode of production. That said, perhaps a target of profit, in spite of that aspect being abstract. And determining the MO. Do you want 15 minutes of fame or 15-fold current profit margin? With baseline data you can assess the impact of cinematography after the fact, for either variable.
-
I want to leave Russia, I want help
Riobard replied to DanyaHULUS's topic in European Men and Destinations
How to think this through? There is the conscientious objector persecution argument, that legitimizes asylum-seeking. However, that impedes running the gauntlet upon departure and any suggestion or fabrication of evidence of implicit or explicit anti-war or anti-Russian sentiment is imperiling. Such a candidate would likely not be producing documentation that asylum has been granted, thereby Russian officials graciously stepping aside. If not a candidate for mandatory conscription it might be easier to cross out of Russia but the basis of claim for asylum-based entry might consequently be less robust, would not be an added factor that compounds other reasons that meet the convention. Paradoxically, the concrete evidence of persecution that underpins a basis of claim is usually manipulatively interpreted by Russian authorities as an undermining of patriotism. I believe that there is typically a scan of evidence and that documentation is best compartmentalized. Phone wiped clean of any declarations of antipathy or desired respite, bearing in mind that any one official might not be doing backflips about staying. That said, Ukrainians and Russians alike share some similarities in legitimacy. I am given to understand that either group is plagued by the necessity of biometric documentation, at least for admission to Canada. -
I want to leave Russia, I want help
Riobard replied to DanyaHULUS's topic in European Men and Destinations
I know somebody, actually barely acquainted, that had the means to leave, for now, just enough for transport out, primarily prompted by the mandate of armed forces conscription in the context of this year’s invasion, the straw that broke the camel’s back already burdened by attitudes of homonegativity and general grass not at all green reality. Thriving elsewhere without resources is a major challenge. I am not up to speed on impediments to leaving the country if one has not completed military service while not exceeding the upper limit of age for the draft. -
Just to be clear, my Bogotá Monkeypox case prevalence estimate of approximately 1 in 100 intimacy candidates is based on official reports of current rolling case incidence, adjusted for Bogotá proportionality of national figures as well as consensus regarding proportionality of susceptible MSM within overall general populations, and a conservative estimate of on-average 10 days of individual case contagion. It does not account for possible undercount because the ratio of true incidence to diagnosed incidence is not known. Therefore, my estimate is actually conservative overall. If case undercount is a genuine phenomenon, then the point prevalence increases upward from 1/100 to the extent that the current officially reported case incidence is inaccurate. For example, 3 undiagnosed cases, for every diagnosed case that underpins surveillance figures, alters the overall Bogotá MSM setting point prevalence estimate to 1 in 25-ish. Ironically, the opinion that undercount is a feature that supports the relatively innocuous consequences of this virus, as believed by some, just inflates estimates of point prevalence. If those estimates represent ‘fear porn’ to some attempting to interpret risk, then the assertion that there is a tip:iceberg ratio is where the finger-pointing regarding alarmism more appropriately lands. What is important is knowing probability of cases and associated transmission potential in specific contexts. Thereafter every individual must assess their particular infection risk tolerance. The clinical consequences are fairly well known. I would not presume to either minimize or exaggerate those consequences. It is mystifying that a reader would obnoxiously object to epidemiological data reporting because the magnitude of prevalence appears to him to contradict his subjective view of the magnitude of morbidity impact. The trend of decline in incidence may eventually emerge in Colombia that seemingly arrived late to the party. If the disease peters out, say, because 75% of MSM infections are dispersed by 25% of those MSM and the latter achieves higher rates of recovery and/or vaccination immunity that in turn reduce ongoing transmission all that will have been a reassuring good thing that happened because a bad thing preceded it. The anticipation of absence of incidence recidivism in specific locations actually supports the idea of capitulating to a transient adjustment in travel plans. That is hardly at the level of being perpetually startled by one’s shadow.
-
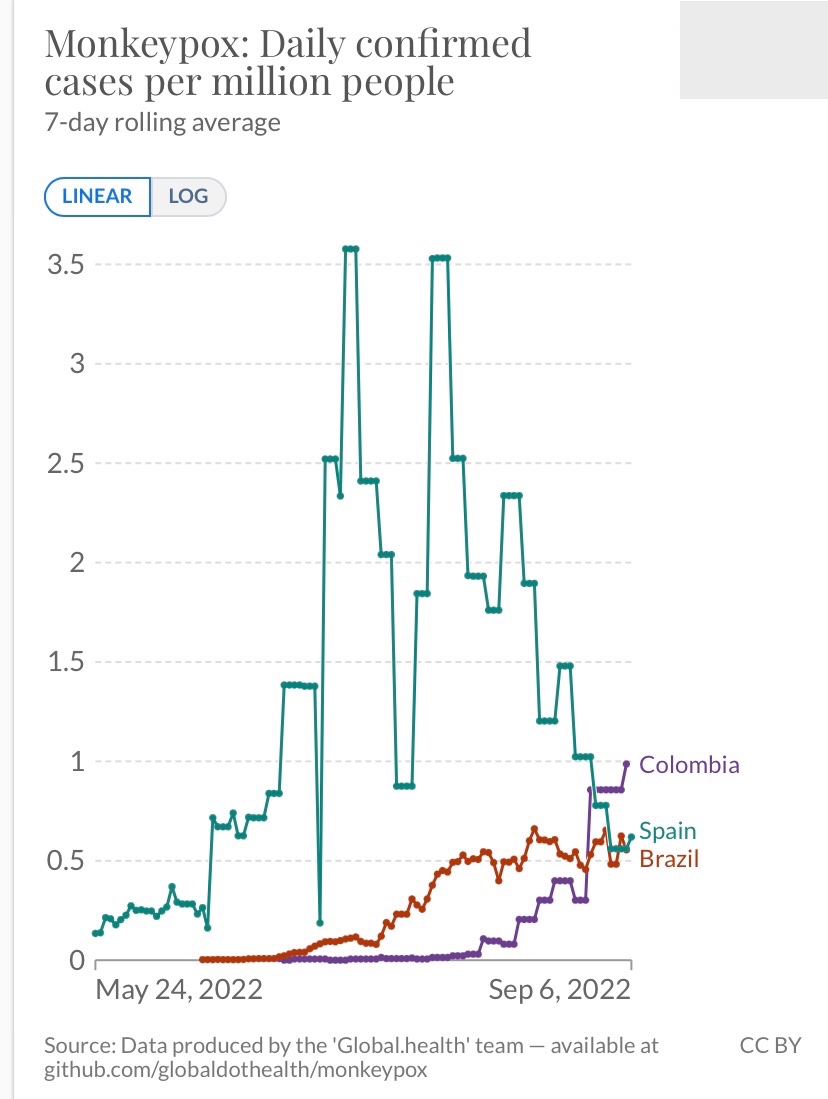
No need to hyperventilate. Take your Facebook U credentials to Twitter rants. LOL My figures are correct based on MSM population share denominators and duration of case transmissibility. You seem to be manufacturing testing and reported:true incidence data to make a point regarding your subjective take on the gravity of the situation and to project hysteria on another’s simple rendering of objective facts that would undermine a vacation if simple bad luck were to occur, a trip that is postponable, at a fairly definable degree of probability in the context of commercial sex trade in particular, that sex tourism mode additionally located in the sleazy person-congested indoor settings we have grown to love. There is nothing you can teach me about Infectious Diseases that I don’t already grasp. I have actually written nothing on this forum about Monkeypox morbidity and mortality. I have myself pointed out the substantial drop from peak case incidence in Spain. Yes it is correct that, for example, in Spain MVA-BN uptake at merely about 5% the target susceptible MSM subpopulation has been followed by a steep case incidence decline evidently heading to its first nadir. To what extent shifts in occurrence are attributable to vaccination, pathogen self-limiting factors, etc, are unclear. There is nothing overreactive about aiming to strategize one’s timing of trips to hopefully coincide with lowered disease risk according to infection prevalence trends that are usefully available according to public health surveillance over time. That is simply an additional slice of Swiss cheese added to the stack that includes other tried and true behavioural risk mitigation measures at our disposal, aiming to prevent a seeping through of a mishap that ruins a trip. I caught dengue in Brazil. It destroyed a pricey vacation. The transmission chances are very low. I return repeatedly. If 1 in 100 mosquitoes bites in Rio de Janeiro were to be accompanied by a fair probability of gifting dengue in spite of common sense attempts to reduce exposure, if it could actually be reasonably quantified, it would give pause.
-
So my friend in Rio has Monkeypoxx
Riobard replied to bucknaway's topic in Latin America Men and Destinations
Erratum above: should be ignore the hatch between the first two vertical bars. -
So my friend in Rio has Monkeypoxx
Riobard replied to bucknaway's topic in Latin America Men and Destinations
I read the preprint a few days ago. Tellingly, the MPXV-specific antibody titres for the younger group after two MVA-BN doses (red asterisk) never nearly reach those of the pre-MVA-BN but historically Smallpox-vaccinated (yellow asterisk). So if antibody level is the main protective immunity factor the logic is that older Vaccinia-experienced would do no more poorly if not receiving MVA-BN in the current outbreak. However, many older guys got symptomatic infection prior to MVA-BN rollout and that would logically lead to the conclusion that recently vaccinated younger guys could get breakthrough infection. What remains to be seen is the comparative infection breakthrough potential between the two groups. Also, if antibody titres are the key, and if the lower quantities for younger actually satisfy the threshold for protection, then these results lead me to believe there is not much point in 2nd dose uptake for me if such is offered in Canada. (Ignore the black hatch sitting between the first two horizontal bars; it’s a smudge I realized I accidentally made when editing the photo.)
-
So my friend in Rio has Monkeypoxx
Riobard replied to bucknaway's topic in Latin America Men and Destinations
Yeah T Yeah, Titanji is often interviewed but she tends to skip over the points about DRC case surveillance that are formally referenced in most MVA-BN product guidance. There is macaque response, yes/no dichotomous serological conversion in human studies with a % rate, magnitude of antibodies generated in human studies, and finally but not MVA-BN related the DRC surveillance I mentioned, which is the basis of the metric ‘up to 85%’, an inference from Smallpox vaxx history. Many moving research parts that get conflated with one another. -
No adverse reaction to one standard MVA-BN dose, on top of the possible benefit of having had Smallpox vaccination some 6 decades back. Reservations relate to commonly accepted uncertainty about MVA-BN protectiveness. Also, without vaccine supply in Colombia an exponential incidence surge could temporarily shut down where I intended to be naughty by the time I arrive, possibly as case incidence is peaking.
-
Well said. My deeply researched and experience-based (past in Bogotá) playbook was to have been strictly tourism outside of Bogotá. Exclusively venue-curated play, ie, St Moritz baths and Gigolo club upstairs when in Bogotá 3 nights. My decision rests on postponing due to those two congregate setting risks and leaving only airfare on the table versus a possible abstinent couple of weeks. I don’t hire from ads.
-
Tarnation, I have a trip planned this month with a sexual play focus within the Bogotá component, where majority Monkeypox incidence for the nation is located, but have been holding off on accommodations for the entire trip, in case this … and also minimal vaccine supply there. I estimate the daily Bogotá MSM incidence at 1/1,000, contagion point-prevalence at about 1/100 MSM.
-
So my friend in Rio has Monkeypoxx
Riobard replied to bucknaway's topic in Latin America Men and Destinations
The 85% referenced is not from animal models. It is drawn from dated MPXV outbreak attack rates in Democratic Republic of Congo comparing VARV (Smallpox) vaccinated to those younger and unvaccinated. The assumption being that the later MVA-BN derivative from earlier iterations of vaccine is likely as effective.